A 60 year old male came with severe head ache
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 60 year old came to opd with severe headache
Chief complaints
Severe headache since 5 days
Hopi
Patient was apparently asymptomatic 5 days back then he developed headache , so he visited local RMP and diagnosed with hypertension ( 160/100) then he had local medicines. The next day BP was high so he was asked to refer to higher centre.yesterday his BP was 200/110 when he came to our hospital.
Neck movements are restricted since 5 days
No h/o fever
No h/o vomitings
Past history
No h/o DM,CAD, epilepsy,thyroid,asthma,TB
History of fracture to right arm
Daily routine
Patient gets up at 4 am and does he daily chores ,have breakfast at 9 am (rice , vegetable curry,tea) and goes to his daily labour work.he ll have his lunch at work and comes back to home at 5pm .he ll have alcohol(. 90ml)daily night and have his dinner at 9pm and sleeps at 10pm.
Personal history
Appetite: normal
Diet:mixed
Bowel: normal
Bladder:decreased frequency
Addictions: alcohol and beedi(daily 5 )
General examination
Patient is conscious,coherent,cooperative ,well oriented to time, place and person.


Video of restricted neck movement
https://youtube.com/shorts/Alw-93VZ9G8?feature=share
Pallor: absent
Icterus: absent
Clubbing:absent
Cyanosis:absent
Lymphadenopathy:absent
Pedal edema: absent
Vitals
BP: 180/100
PR:70bpm
Temp: afebrile
RR: 16
Systemic examination
CVS - S1 S2 heard
R/S - inspection
No scars present
Trachea- central
Auscultation:
Vesicular breath sounds heard
P/A -
Inspection - Umbilicus inverted , No abdominal distention,scars and swelling.
PALPATION: Soft, non tender, no organo megaly.
AUSCULTATION:
BOWEL SOUNDS HEARD
CNS - NO focal deficit found.
No meningeal signs
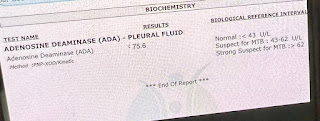
Investigations


USG

Provisional diagnosis
Hypertensive urgency


Comments
Post a Comment