This online E-log Entry Blog is an objectively structured clinical examination method to assess the clinical competence during the course of my General Medicine Internship rotation (october'2023-november'2023) by reviewing the case reports shared below and to discuss, understand and review the clinical scenarios and data analysis of patients so as to develop my clinical competency in comprehending clinical cases, and providing evidence-based inputs for questions surrounding the clinical vignettes borrowed from the E Log Book.
Note: The cases have been shared after taking consent from the patient/guardian. All names and other identifiers have been removed to secure and respect the privacy of the patient and the family
This is a case where I presented in the CME meet :
A 47 year old male patient came to casualty with chief complaint of spasms of both upper and lower limbs since one day
HOPI:
Patient was apparently asymptomatic one day back then he developed spasms in his both upper and lower limbs which was sudden in onset gradually progressive . No aggravating and relieving factors.
History of perioral numbness, easy fatiguability.
No history of tonic clinical movements
No history of loss of consciousness
No history of bladder / bowel incontinence
No history fever, nausea and vomiting
No history of shortness of breath
No history of cold and cough
No history of loose stools.
History of similar complaints in the past( 5 years ago ) with chief complaints of sudden onset of weakness of all four limbs which progressed to complete weakness in 3 days for which he got admitted in the hospital and got treated accordingly.
PAST HISTORY:
K/c/o Hypertension since 6 years on unknown medication
Not a known case of DM, Asthma, TB, Epilepsy, CAD, CVA,
and Thyroid Disorders.
PERSONAL HISTORY:
Moderately built and Moderately nourished.
Appetite- normal.
Sleep -adequate.
Diet- mixed.
Bowel and bladder movements regular.
Addiction- Alcoholic since 20 years (consumed approximately 360ml of alcohol per day since 10 days due to elections)
FAMILY HISTORY :
No relevant family history
GENERAL EXAMINATION
Patient was conscious, coherent and cooperative
Patient was anxious at the time of admission
No signs of pallor , cyanosis , icterus , clubbing , lymphadenopathy , generalised edema
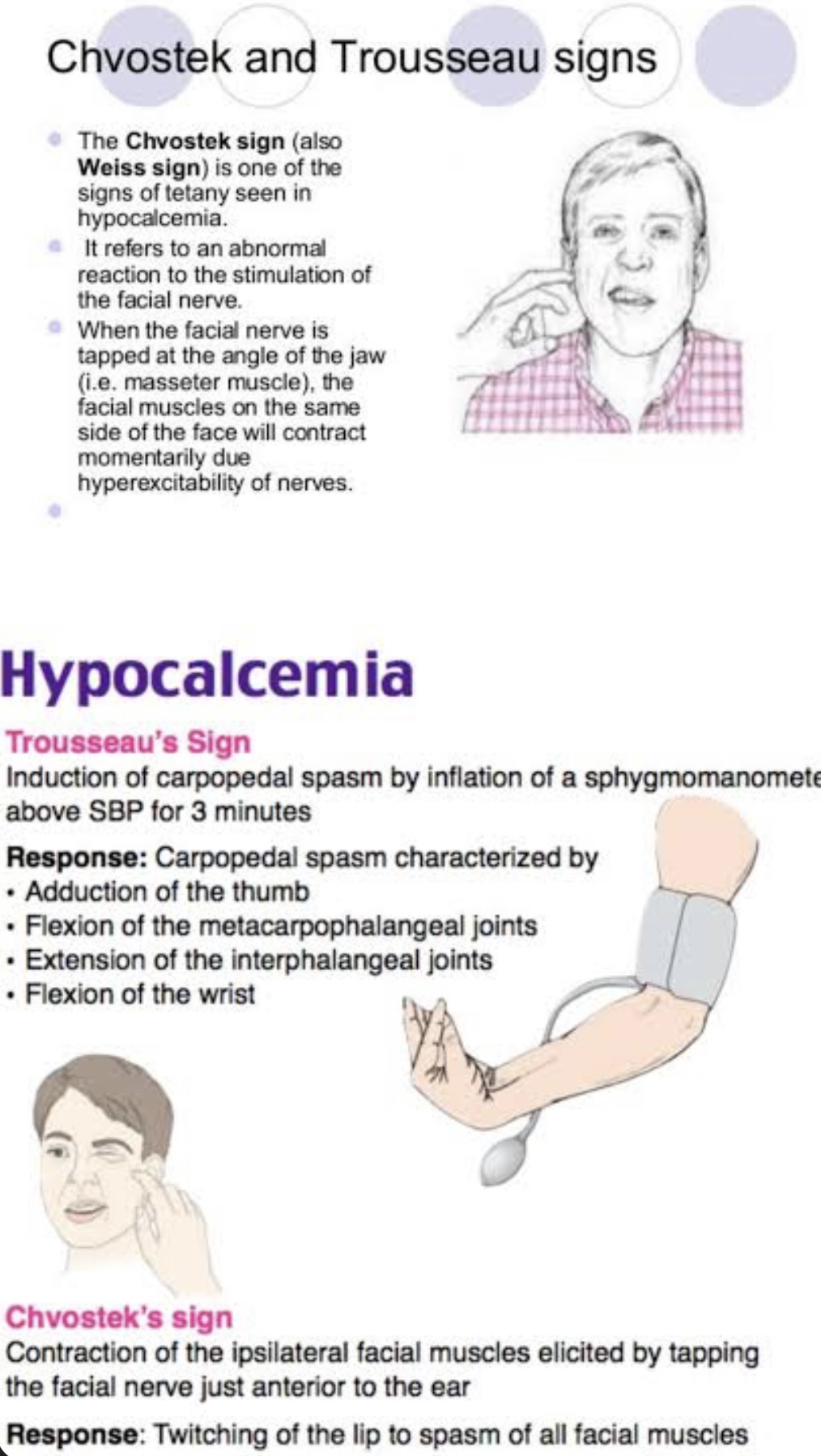
Trousseau sign was present
Chvostek sign was present
Vitals -
Temperature: 98. 4 °F
PR : 92 bpm
BP : 150 /80 mm of hg
RR : 28 cpm
SpO2 : 98% on room air.
GRBS : 98 mg /dl
SYSTEMIC EXAMINATION
CNS :
Level of consciousness-alert
Speech - normal
Cranial nerves function- Normal
Motor system:
Right Left
Power. UL. 5. 5
LL. 5. 5
Tone. UL. Normal. Normal
LL. Normal. Normal
Reflexes.
Biceps. ++ ++
Triceps. ++ ++
Supinator. ++ ++
Knee. ++ ++
Ankle. ++ ++
Sensory System : Normal
CVS : S1S2 heard , No murmurs heard
RS : Bilateral air entry clear
Per abdomen : soft and non tender, bowel sounds heard
PROVISIONAL DIAGNOSIS :
TETANY FOR EVALUATION
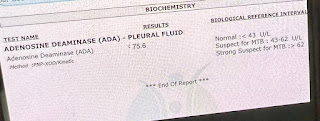
Investigations :
ABG
PH - 7.62 (normal 7.32-7.45)
PCO2- 19.5 mmHg(normal 35-45)
Po2 - 106 mmHg ( 85-95)
HCO3- 20.7 mmol/l (22 - 26 mEq/L)
SO2: 97.7%
Na+: 132 mmol/L
K+ : 2.7 mmol/L
Ca+2 : 0.47 mmol/L
FINAL DIAGNOSIS:
TETANY SECONDARY TO RESPIRATORY ALKALOSIS
Treatment
Rebreathing mask
Inj. Calcium gluconate 2 g in 100 ml NS over 15 min
Inj. KCl 40 mEq + 500 ml NS iv over 6 hrs
Tab. Telma H PO/ OD
Osce questions:
What is relation between respiratory acidosis causing hypocalcemia?
Respiratory alkalosis is an elevation in pH secondary to reduced arterial partial pressure of carbon dioxide (pCO2) in the setting of hyperventilation. It can be either acute or chronic and is the most common acid-base disturbance in critically ill patients. Hyperventilation often leads to hypocapnia, which in turn leads to a slight reduction in bicarbonate, hypokalemia, and hypophosphatemia due to an intracellular shift of potassium and phosphate, and hypocalcemia due to increased calcium binding to albumin in the setting of increased pH.
Can alcohol cause hypokalemia?
Yes, alcohol can affect your potassium levels. Consuming large amounts of alcohol can cause your body to excrete potassium in the urine. This can lead to decreased potassium levels in your bloodstream.
Furthermore, drinking excessive amounts of alcohol can cause dehydration which can cause the levels of potassium in your body to become dangerously low. Additionally, the consumption of some alcoholic beverages, such as cocktails and beer, provides large amounts of simple sugars, which can result in an increase in potassium retention in the body.
Alcohol dependence vs alcohol abuse?
Alcohol dependence causes people to keep drinking to avoid experiencing withdrawal symptoms. Alcohol abuse, on the other hand, involves drinking excessively without having a physical dependence. Both have serious health risks.While the two are no longer differentiated in the DSM, understanding their original definitions can still be helpful.
Alcohol dependence:
Alcohol dependence was originally defined as a chronic medical condition characterized by experiencing symptoms of withdrawal when the person stops consuming alcohol. To avoid experiencing withdrawal symptoms, the person has to keep consuming alcohol
Alcohol abuse:
Alcohol abuse was defined as a condition in which a person continues to drink despite recurrent social, interpersonal, health, or legal problems as a result of their alcohol use.A person who abuses alcohol may also be dependent on alcohol, but they may also be able to stop drinking without experiencing withdrawal symptoms.
Learning points:
Eliciting chcostek sign and trousseau’s sign
Respiratory alkalosis vs acidosis
ABG interpretation: as
In the rotations of medicine department I’ve assisted in central line
Learnt about 2d echo machine techniques
PAJR group links of the cases I’ve worked on:
https://chat.whatsapp.com/KXzmKmNwqXgHkcwxOhfmfW
https://chat.whatsapp.com/FRrAC1DK3OR7xbhiaJHMxH
Showing areas to search in image







Comments
Post a Comment